Name:G. Jagadeesh. DATE:24/07/2021.
Roll No:37.
3rd semester
Hi,
E log is a platform for patient -Centered case in learnings medicine . Hope this will be informative .
Q ) 1.
This is a peer review of the previous assignment by Tejaswi enduri (36) .
https://tejaswienduri.blogspot.com/
Q1) She have did a marvellous job in choosing and examining different cases (10) . She gave an overview onthe treatment and graded them. she had also looked into symptomatology and explained the treatement.
Q2)she had did a case on TRANSVERSE MYELITIS.
Chief complaint provided isnpain on passive movement of the hip.
The patient was asymptomatic 3days back.
she was not able to walk last night.And she had no history of DM,HTN,CAD,Asthma,TB,epilepsy.no simi;ar complaints in past.Has no known allergies and addictions.
there is no specific treatement history.Upon general examination she was found to be no pallor,icterus,cyanosis,clubbing,lymphadenopathy.
Vitals were normal except temperature was afebrile.
tests done are
SERUM ELECTROLYTES.


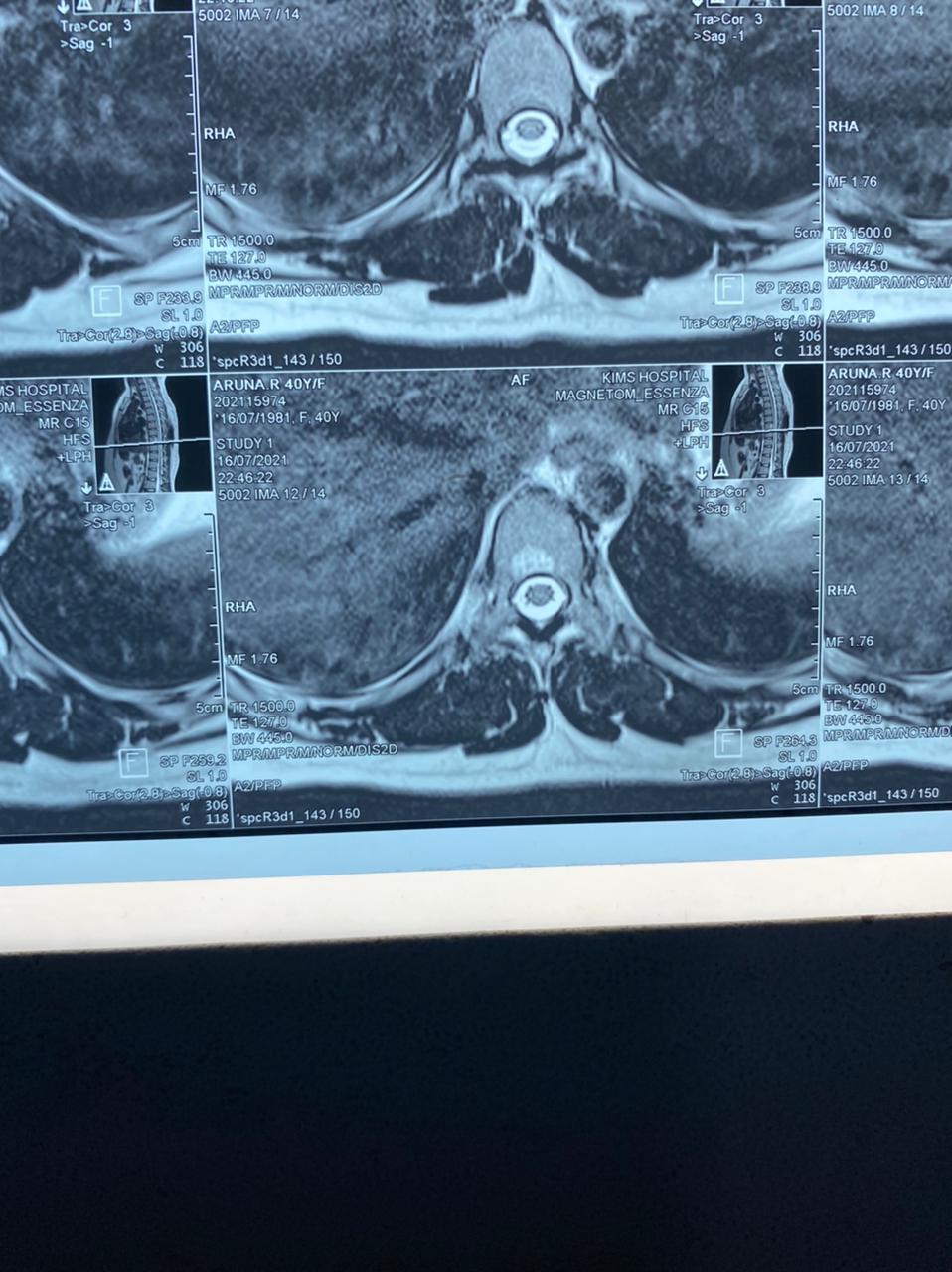





 MRI SCAN.
MRI SCAN.

3)SERUM ELECTROLYTES





8)PROTHROMBIN TIME


ECG, RFT, CUE, Hemogram, ABG , Serum electrolytes, Blood urea ,USG Abdomen ,LFT
13/7/21 USGABDOMEN AND PELVIS
CUE,ABG,S/E
ECG

BLOOD UREA

SERUM CREATININE
COMPLETE BLOOD PICTURE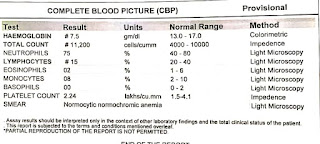
SERUM URIC ACID
URINE CULTURE

BLOOD CULTURE
SERUM ELECTROLYTES










PHOSPHORUS

SERUM CALCIUM
 Colour dopler -2D Echo
Colour dopler -2D Echo
Tests done on 17/7/2021
 CBP
CBP MRI-SPINE
MRI-SPINE
 Investigations done on 19/7/21CBP
Investigations done on 19/7/21CBP
INVESTIGATIONS DONE ON 21/7/21Pelvis-AP view Bacterial culture report
Bacterial culture report  CBP
CBP
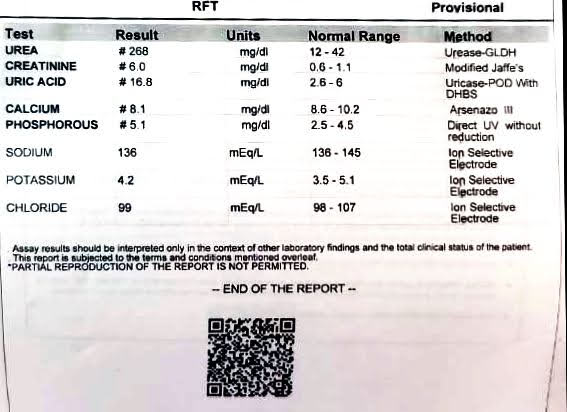
INVESTIGATIONS DONE ON 22/7/21Hemogram  Blood urea level is so much high which should have been maintained by normal kidneys.Hb level was decreased may be due to loss of Hb through kidneys.The main thing is there is decreased creatinine clearence.CREATININECreatinine is an endogenous athreshold substance for kidney which should be excreated in urine.creatinine is formed by LOHMANN REACTION.
Blood urea level is so much high which should have been maintained by normal kidneys.Hb level was decreased may be due to loss of Hb through kidneys.The main thing is there is decreased creatinine clearence.CREATININECreatinine is an endogenous athreshold substance for kidney which should be excreated in urine.creatinine is formed by LOHMANN REACTION. The creatine formed here undergo some spontaneous reactions which leads to formation of CREATININE.EXCREATION OF CREATININE.Creatinine is cleared from plasma by GFR.and there is also some secreation by tubules into the lumen and creatini ne excreation takes place.so if there is problem with creatinine clearence then we can expect renal failure.
The creatine formed here undergo some spontaneous reactions which leads to formation of CREATININE.EXCREATION OF CREATININE.Creatinine is cleared from plasma by GFR.and there is also some secreation by tubules into the lumen and creatini ne excreation takes place.so if there is problem with creatinine clearence then we can expect renal failure. Treatement and prophylactic treatemebt was given and it is nice.she had presented a case on CKD.it was good but there are no perfect reports posted in log book.but the treatement was good based on investigation done.LFT says that bilirubin levels are increased , enzyme panel is also disturbed RFT says that UREA,URIC ACID and CREATININE LEVELS are abnormal indicating renal failure.treatement is good and satisifactory.Now at present the patient have shifted to ORTHOPAEDIC DEPARTMENT.She had presented a case on diabetes with breathlessness.the patient was also suffering from fever and diarrhoea.the patient is diabetic since 4 years.General examination and systemic examination was found to be normal.VITALSfluctuation of BP.temperature was afebrile.INVESTIGATIONS DONE ARE
Treatement and prophylactic treatemebt was given and it is nice.she had presented a case on CKD.it was good but there are no perfect reports posted in log book.but the treatement was good based on investigation done.LFT says that bilirubin levels are increased , enzyme panel is also disturbed RFT says that UREA,URIC ACID and CREATININE LEVELS are abnormal indicating renal failure.treatement is good and satisifactory.Now at present the patient have shifted to ORTHOPAEDIC DEPARTMENT.She had presented a case on diabetes with breathlessness.the patient was also suffering from fever and diarrhoea.the patient is diabetic since 4 years.General examination and systemic examination was found to be normal.VITALSfluctuation of BP.temperature was afebrile.INVESTIGATIONS DONE ARE
 Abdominal examination :
Abdominal examination :- Soft
- Non tender
- No palpable masses
Cns examination :- Unconscious / altered
- Speech no response
- No signs of meningeal irritation
- GCS (coma scale) :E 3 V 4 M 5 ( before arrest )
- After arrest E 1 V T M1
- Yesterday also same GCS
- Today E1 V T M4
Provisional diagnosis: DKA with AKI ( ? Pre renal) USG(25/06/21) - Pyelonephritis.
Laboratory investigations :ABG analysis:Day 1
Day 2)ABG analysis
Complete blood picture 
Liver function tests:
 Kidney function tests :
Kidney function tests :
 Based on the above results, she was put on dialysis by afternoon 2pm. Day 3
Based on the above results, she was put on dialysis by afternoon 2pm. Day 3 





 Day 4
Day 4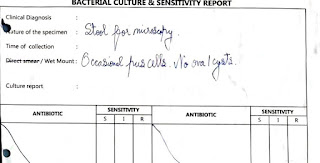


 Day 5Post dialysis reports
Day 5Post dialysis reports
 Hb Is less.
Hb Is less.
 Increased level of creatinine and uric acid.
Increased level of creatinine and uric acid.

Day 6 and 7 Bed sores
Bed sores
BP 150/80mmHgPR 89c/mVentilator was disconnectedSpO2 98% on oxygen mask.GCS E4 V1 M4 No change in treatment.


 HE also have diabetes ketoacidosis.
HE also have diabetes ketoacidosis.
LFT says that bilirubin levels are increased , enzyme panel is also disturbed RFT says that UREA,URIC ACID and CREATININE LEVELS are abnormal indicating renal failure.treatement is good and satisifactory.Now at present the patient have shifted to ORTHOPAEDIC DEPARTMENT. the case is diabetic nepropathy.History was taken good .General examination and systemic examination were normal.VITALSTemperature is afebrile and other were normal.INVESTIGATIONS DONRE ARE.




17June 2021

21June

25June


28 June





14 April to 27 April 2021



21 May 2021





Temperature charting
 Urine bag with plenty of pus cells on 22nd may 2021
Urine bag with plenty of pus cells on 22nd may 2021

Urine bag on 31 May 2021 ( After treatment)



- Soft
- Non tender
- No palpable masses
- Unconscious / altered
- Speech no response
- No signs of meningeal irritation
- GCS (coma scale) :E 3 V 4 M 5 ( before arrest )
- After arrest E 1 V T M1
- Yesterday also same GCS
- Today E1 V T M4




 Based on the above results, she was put on dialysis by afternoon 2pm.
Based on the above results, she was put on dialysis by afternoon 2pm. 










 Hb Is less.
Hb Is less. Increased level of creatinine and uric acid.
Increased level of creatinine and uric acid.


















14 April to 27 April 2021











Xray

NCCT KUB

HYDRONEPHROSIS



 Investigations done are good and treatement was also good.Q5)The online learning is not that satisifactory.
Investigations done are good and treatement was also good.Q5)The online learning is not that satisifactory.







Comments
Post a Comment