82F with bilateral knee joint pain and Fever
Hello all this is G Jagadeesh,a eight semester student.This E Log depicts the patient centered approach to learning
This is an online e log book to discuss our patient de-identified health data shared after taking his/her/guardians signed informed consent. Here we discuss our individual patient problem through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evidence input.
I have been given this case to solve in an attempts to understand the topic of patient clinical data analysis to develop my compentency in reading and comphrending clinical data including history , clinical finding , investigation and come up with diagnosis and treatment plan....
This is the case of an 82-year-old female who presented to the hospital with chief complaints of
- Pain in the lower limbs since 2 days, bilaterally
- Fever since 2 days
- Swelling in the lower limb, bilaterally since 2 days
History of Presenting Illness
The patient was apparently asymptomatic 6 months ago.
6 months ago, the patient experienced a pricking type of joint pain while climbing the stairs, it was pricking in nature, and the patient could carry out her daily activities without hindrance.
In a matter of three days, the patient developed a sudden onset of pain. The pain was pricking in character, and continuous. present bilaterally in the lower limbs at and below the level of the knee. It aggravated on walking and relieved at rest.
The pain was associated with swelling of the lower limb at and below the level of the knee joint, bilaterally. It was associated with redness over the limbs.
The patient also experienced high-grade fever, which was continuous, and . not associated with chills and rigour. She also experienced generalised body pain and malaise.
2 Days later, the patient visited a doctor and was prescribed medications. The symptoms reduced after the consumption of medicines.
One week later, there was a sudden increase in pain and swelling similar to the last episode. There was also a rise in fever up to 104 degrees Fahrenheit.
The patient came to our hospital and was given, NSAIDS, paracetamol,normal saline and antibiotics. This resulted in a reduction of symptoms, and the patient was discharged.
2 Days later, the patient developed the same constitution of symptoms again and came to our hospital.

Past History and treatment history
The patient is a known case of hypertension since 10 years and has been on Telmisartan and Amlodipine since then.
10 years ago, the patient had a history of trauma, that led to a fracture of the ulna.
8 Months ago, the patient had a syncopal attack and was started on low-dose aspirin as a prophylactic measure.
The patient is not a known case of Diabetes Mellitus, Tuberculosis, CAD, or Epilepsy.
The patient consumed NSAIDs when she experienced pain.
She was prescribed Diethyl Carbamazine, on her first visit to the doctor since 15 days.
She was prescribed amoxicillin seven days ago.
Family History
Brother and sister have asthma.
Personal History
Appetite: reduced since yesterday
Diet: Vegetarian
Sleep: The patient consumes alprazolam (on prescription) as she has difficulty falling asleep.
Bladder: 9 months ago, the patient had oliguria, since the onset of fever, she has increased the frequency and urgency of micturition.
Bowel Movements: Normal
Addictions: None
Allergies: none.
General Examination
The patient is conscious, coherent, and oriented to time, place and person.
The patient is moderately built and moderately nourished.
Vitals :
- Pulse - 94 beats per minute
- RR- 16 cycles per minute
- Temperature: Afebrile
-Blood Pressure- 120/70 mmHg
Pallor - Present

Icterus - absent

Cyanosis - Absent


Clubbing - Absent

Koilonychia - absent
Lymphadenopathy - Absent
Oedema -present

Peripheral pulsations were felt in the dorsalis pedis, anterior and posterior tibial arteries, and radial arteries.
Examination of the Musculoskeletal System
Inspection findings -
Bilateral swelling of the lower limbs, at and below the level of the knee joint. More prominent on the right than the left.
Right, Limb Fixed flexion deformity seen at the knee joint.
Left lower limb, ability to flex knee present.
No scars, sinus, erythema or rashes



Palpatory Findings
Local rise of temperature present bilaterally on the knee joint
Palpable swelling is present on the right and left knee, and ankle with mild oedema in her lower limbs , associated with tenderness, in the suprapatellar bursa
Patellar tap is positive bilaterally.
Join Line tenderness observed.
absence of lower limb shortening.
Range Of Motion
Inability to flex the left lower limb.
Upper limb Findings
Inspection
-4th metacarpal hyperextended. In the right hand .

Palpatory
- no tenderness
Range of motion
- reduced.
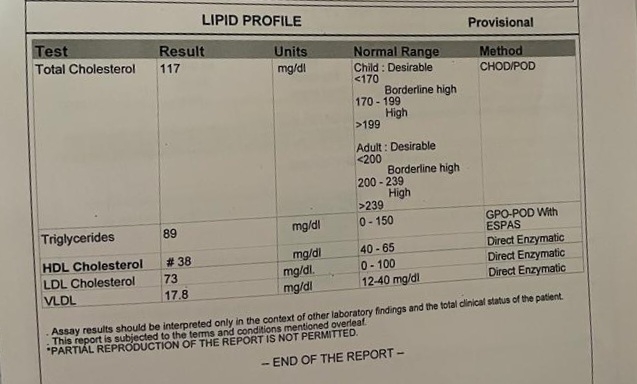
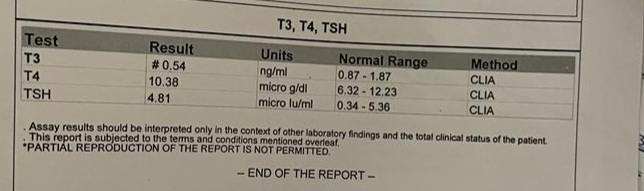
Investigations












? Bursitis
? Osteoarthritis




Treatment admission 3 ;
Neomol, telmisartan, paracetamol, orofer,Ultracet, shelcal
Diagnosis :
Pyrexia with polyarthralgia with iron deficiency anemia



Comments
Post a Comment